da Vinci Sacrocolpopexy is a procedure in which the surgeon utilizes a robotic platform to assist in the surgical correction of pelvic organ prolapse. The robotic platform allows the surgeon to control a 3D camera and three robotic arms that are introduced through small incisions in the abdomen. An assistant is also at the patient’s bedside throughout the procedure to assist the surgeon through a separate small incision.
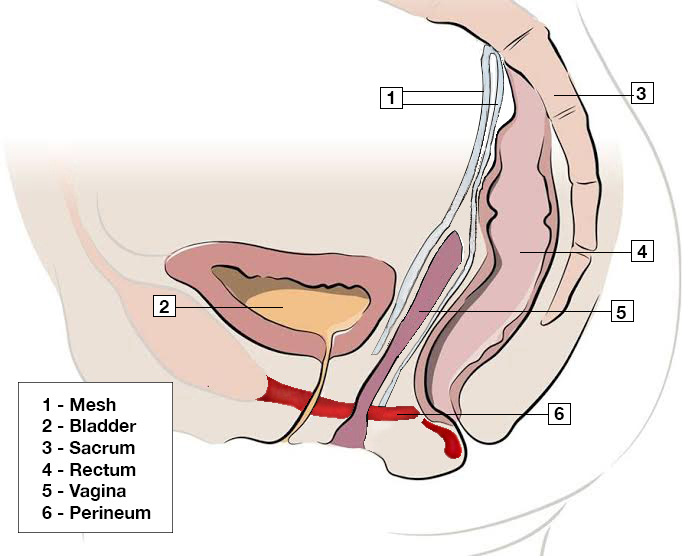
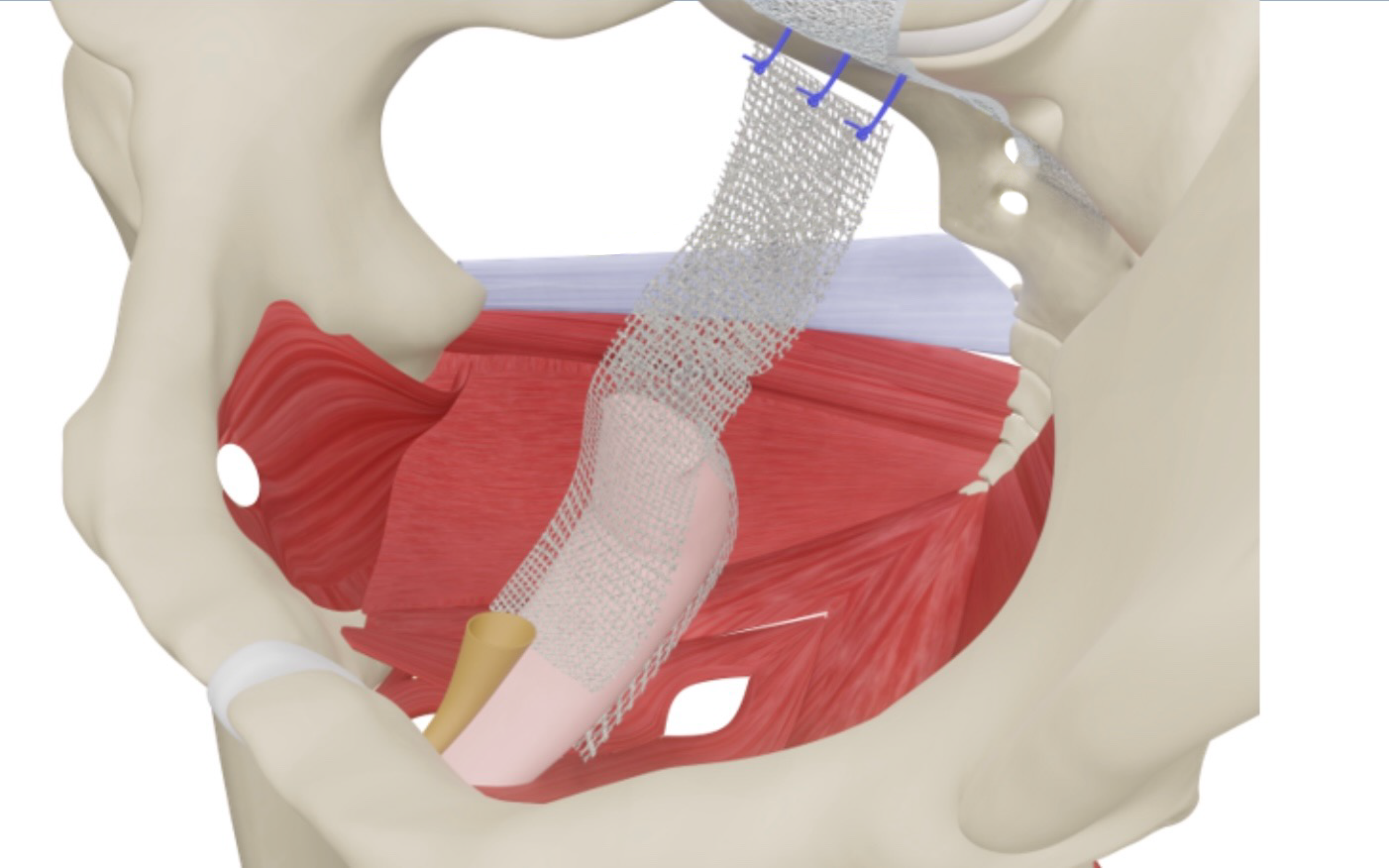
During the sacrocolpopexy procedure, two strips of polypropylene mesh are tailored to the patient’s prolapse. One mesh segment is sutured into the space between the bladder and the vagina and the second mesh segment is sutured into the space between the rectum and the vagina. The mesh is also attached to the top of the vagina or cervix. The other ends of the mesh segments are sutured to the sacrum. This elevates the entire vagina, correcting cystocele, rectocele, and enterocele.
In patients who also have perineal descent and vaginal relaxation or looseness, sacrocolpoperineopexy is performed. Sacrocolpoperineopexy is essentially the sacrocolpopexy procedure (described above) combined with vaginal reconstructive surgery.
With this approach, the pelvic floor musculature is lifted, the perineum is rebuilt and the vagina is tightened. Vaginal tightening is also referred to as vaginal rejuvenation. Vaginal rejuvenation is done to treat symptoms of looseness and associated decreased sensation with intercourse.
Dr. Shashoua has been performing open abdominal sacrocolpopexy since 1995 and da Vinci sacrocolpopexy since 2007. Most sacrocolpopexy surgeries are now performed with the da Vinci robot. Dr. Shashoua performs around 3-5 sacrocolpoperineopexy procedures a week. Patients typically are discharged from the hospital on the day following the procedure and return to normal activity in 2-3 weeks. Healing is for the most part complete 6 weeks after surgery.
Book An Appointment
My treatment was the Da Vinci Sacrocolpoperineopexy and Mid-Urethral Sling, with surgery being performed by Dr. Shashoua and his staff at Austin Urogynecology. My conditions I dealt with were Cystocele, Rectocele, Pelvic Organ Prolapse and Urinary Incontinence… When I could no longer ignore the several conditions I was struggling with any longer, I was referred to Dr. Shashoua's office. …I am now past my six week follow-up and feel great. It is wonderful to cough and sneeze or jump around without leakage! I never had much pain from the surgery and after post-op check-up, was up and around with no problems. Dr. Shashoua and his staff have always been the best. So sincere and willing to answer any and every question you have. They all have been so informative, and have provided information when I didn't know what questions to ask. I feel very fortunate that I was directed toward Dr. Shashoua at Austin Urogynecology. Thank you so much Dr. Shashoua!
-Susan P.
Transvaginal Mesh Concerns
“Transvaginal mesh,” which was introduced in the early 2000’s to treat vaginal prolapse, has received much attention since the FDA first cautioned against its use in 2008. This culminated in the recent removal of the remaining transvaginal mesh from the market by the FDA in April 2019. There has been some confusion over the type of mesh that the FDA banned and the mesh that is still approved for the treatment of pelvic organ prolapse. The mesh used for sacrocolpoperineopexy is NOT transvaginal mesh as it relates to the FDA’s concerns regarding mesh. The polypropylene mesh we use in sacrocolpoperineopexy is the gold standard for definitive treatment of pelvic organ prolapse.
Complications during sacrocolpoperineopexy are uncommon but can include bladder/bowel injury, bleeding, infection and post-operative voiding dysfunction. Even less common post-operative issues can include vaginal pain or pain with intercourse. Any time there is mesh material placed within the vagina, there is a potential risk of mesh exposure. If the mesh is placed in the appropriate anatomic plane, the risk is low, but can occur if the vaginal incision does not heal properly. This may require reoperation or partial mesh removal.
Got questions? Need an appointment? We’re here to help!
{kind=link}